Abstract
Summary: We describe a remodeling technique in which two compliant balloon catheters were used to treat large, wide-necked bifurcation aneurysms distal to the circle of Willis in two patients with subarachnoid hemorrhage. Although vasospasm and interaction between the constrained catheters in the small distal arteries added to the complexity of the procedure, placement of a balloon catheter in each side branch prevented coil encroachment and enabled embolization of these aneurysms.
Coiling of wide-necked aneurysms at vascular bifurcations remains as a fundamental problem in interventional neuroradiology (1). Modification of the standard techniques of endovascular treatment of aneurysms may be needed to treat some complex aneurysms (1, 2).
Case Descriptions
Case 1
A 56-year-old woman presented with Hunt-Hess grade III subarachnoid hemorrhage and a left sylvian hematoma extending into the left basal ganglia. A cerebral angiogram demonstrated a large aneurysm that incorporated both trunks of the left middle cerebral artery (Fig 1A). A small aneurysm of the anterior communicating artery was incidentally noted. Because of the patient’s poor grade and bad general medical condition and because of the surrounding hematoma, surgical treatment was not favored, and the patient was referred to our department for endovascular treatment.

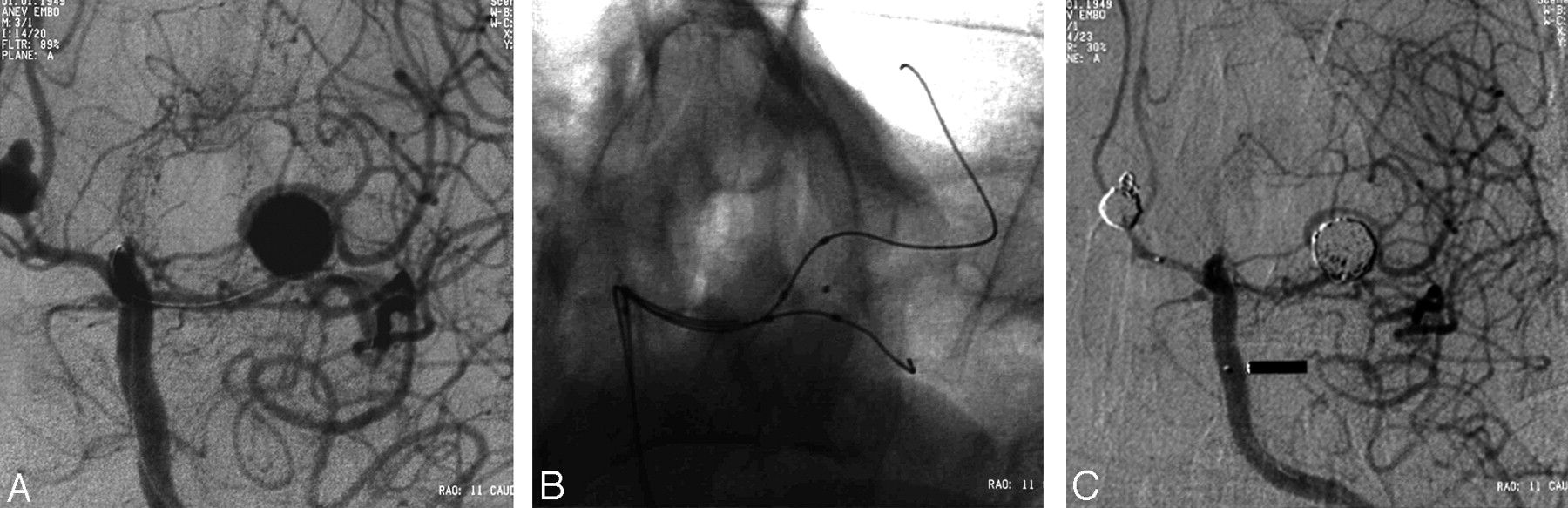
Case 1.
A, Left internal carotid arteriogram (working projection) before bypass of the aneurysm shows that both of the trunks of middle cerebral artery arise from the aneurysm. Microcatheter in the middle cerebral artery and in the anterior communicating artery aneurysm are noted.
B, Digital radiograph shows both catheters (HyperForm; Micro Therapeutics, Inc) in the superior and inferior trunks. Microcatheter tip is in the aneurysm.
C, Left internal carotid arteriogram after embolization of the anterior communicating artery aneurysm shows satisfactory obliteration of both aneurysms.
With general anesthesia and systemic heparinization, 8F and 6F guiding catheters were placed in the left internal carotid artery by means of a bilateral femoral approach. Nimodipine (Nimotop; Bayer AG, Leverkeusen, Germany) 1 mg in 20 mL saline was slowly infused via the 6F guiding catheter to prevent vasospasm (3).
We initially planned to navigate both catheters (HyperForm; Microtherapeutics, Inc, Irvine, CA), each with a proximal outer diameter of 3F (larger than the standard microcatheters for embolization of aneurysms), through the 8F guiding catheter. However, bypassing the aneurysm primarily with the catheter and placing the balloon at the origin of the superior trunk of the middle cerebral artery proved difficult. Therefore, we decided to bypass the aneurysm with a microcatheter (Excelsior SL-10; Target Therapeutics, Fremont, CA) by using a guidewire (Precision 14; Target Therapeutics) and to replace this guidewire with an exchange-length guidewire (X-Celerator 10; Micro Therapeutics, Inc). We used the 6F guiding catheter for this maneuver because it could be placed more distally in the cervical carotid artery than the 8F catheter, and this improved torque control and support for this process.
The 7 × 4-mm balloon catheter was navigated across the neck of the aneurysm to the superior trunk of the middle cerebral artery over the exchange-length guidewire. Another 7 × 4-mm catheter (HyperForm; Micro Therapeutics, Inc) was placed via the 8F guiding catheter, spanning from the M1 segment of the middle cerebral artery to the inferior trunk over a guidewire (X-Pedion 10; Micro Therapeutics, Inc). The aneurysm was catheterized with the microcatheter (Fig 1B).
After selective catheterization of the aneurysm, stagnation of contrast medium was noted in the aneurysm; this resolved with an intra-arterial infusion of 1 mg nimodipine. The aneurysm was coiled during simultaneous inflations and deflations of both balloon catheters. Because this patient with poor-grade disease might have required prophylactic anticoagulation for deep venous thrombosis and concomitant postprocedural hypertension-hypervolemia-hemodilution therapy for vasospasm, the aneurysm in the anterior communicating artery was thought to be at increased risk of rupture and therefore coiled during the same session. The angiogram at the end of the procedure demonstrated satisfactory occlusion of the aneurysms in the middle cerebral artery (Fig 1C) and anterior communicating artery. The patient awakened from general anesthesia at her baseline neurologic condition. Heparinization was reversed after the procedure. Seven days after the procedure, the patient died from septicemia, most likely of pulmonary origin.
Case 2
A 54-year-old patient presented with Hunt-Hess grade I subarachnoid hemorrhage. A cerebral angiogram obtained at another institution 1 week after the subarachnoid bleeding demonstrated a large aneurysm of the anterior communicating artery and diffuse vasospasm. Because of the likelihood of inadequate control of the aneurysm neck during clipping, the patient was referred to our institution for endovascular treatment 16 days after subarachnoid hemorrhage.
With general anesthesia and systemic heparinization, bilateral internal carotid angiograms with simultaneous injections were obtained via a bilateral femoral approach by using 5F and 6F (0.070-in. inner diameter) guiding catheters. The vasospasm had resolved, and both A2 segments were coming off the aneurysm (Fig 2A). Nimodipine, 1.5 mg in 30 mL, saline was slowly infused via both guiding catheters to prevent vasospasm (3). A 7 × 4-mm catheter (HyperForm; Microtherapeutics, Inc.) was navigated from the left A1 to the right A2 through the aneurysm. This maneuver was repeated on the other side to create an X-shaped double-balloon configuration (Fig 2B). The aneurysm was catheterized via the right-sided 6F guiding catheter. With balloons protecting the neck of the aneurysm and both of the proximal A2 segments, the aneurysm was coiled. Postprocedural angiograms demonstrated a residual neck remnant (Fig 2C).

{kind=link}
{kind=link}
Case 2.
A, Aneurysm viewed from its posterior aspect on a 3D angiogram, which shows involvement of the origins of both A2 segments. Small dashed arrow indicates left A1; large dashed arrow, left A2; small solid arrow, right A1; and large solid arrow, right A2.
B, Live road-map image shows the crossed pattern of catheters extending from A1 segments to the contralateral A2 segments and the catheter tip in the aneurysm.
C, Bilateral internal carotid arteriograms at the end of the procedure demonstrate a small neck remnant.
The patient awakened from general anesthesia with mild paresis of left foot, which gradually disappeared after several days. Diffusion-weighted MR imaging demonstrated punctate foci of acute ischemia in the perfusion territory of the left anterior cerebral artery. The patient was given subcutaneous low-molecular-weight heparin for 4 days, which was tapered off in 3 days. He was also given 300 mg/day acetylsalicylate. After his discharge from the hospital on the 12th day after the procedure, the patient had a cerebrovascular accident. An angiogram obtained at 20 hours into the event demonstrated thromboembolic occlusion of the distal left anterior cerebral artery. On discharge, the patient had pronounced right-sided hemiparesis, which gradually improved; however, the patient had a Modified Rankin Scale score of 3 at 4 months.
Discussion
The balloon-remodeling technique had permitted the endovascular treatment of intracranial aneurysms with an unfavorable dome-to-neck ratio (4). In several cases, two balloon catheters were used proximal to the circle of Willis to prevent the encroachment of coils onto the parent artery (5). Despite mastery of remodeling technique in many interventional neuroradiology clinics, endovascular treatment of complex aneurysms in small arteries is still challenging (6). Compliant balloon catheters (HyperForm; Micro Therapeutics, Inc) allow for the treatment of bifurcation and distal aneurysms (6, 7). These balloons can be inflated so that they conform to the neck of the aneurysm (7). However, the neck of an aneurysm may be wider than the length of these balloon catheters. Newer endovascular techniques, such as the placement of two stents to form a Y configuration, have been proposed to treat wide-neck bifurcation aneurysms and to solve the problem of partial protection (1). In some cases, attempts were successful, in others, important complications were observed because of the instability of self-expanding stents or occurrence of thromboembolic events (2, 8, 9).
In our patients, wide-necked aneurysms of the distal bifurcation were treated with two compliant balloons and detachable coils. Surgery was not considered as the first option because of a concern that hematoma might conceal the neck (first patient) or the dome might block access to the neck (second patient) of the aneurysm. Given the possibility of intraoperative rupture, inadequate control of the aneurysmal neck was considered a significant surgical risk, and endovascular treatment was suggested to the patients or their families as first-line treatment.
The advantage of double-balloon remodeling with compliant balloons is that it permits the treatment of wide-necked aneurysms. Side-branch protection and sealing of the neck may be better with this technique than with the single-balloon technique because one balloon is used on each side branch instead of a single balloon bulging into the neck of the aneurysm. Although the simultaneous use of multiple catheters is a potential risk factor for thromboembolic events during coiling (10), the risk may be at least partly offset because the two balloons prevent the encroachment of coils into the parent artery.
The double-balloon remodeling technique has some disadvantages. First, the endovascular space for three catheters is a constraint. Distal arteries of ≤3 mm in diameter cannot easily accommodate three catheters of 2F–3F. We noted that the catheters tended to interact with each other, though they were used through different guiding catheters in both patients. Moving one catheter or inflating a balloon catheter could cause unintended forward or backward movement of the others. Conversely, the presence of one catheter hampered the movement of others during bypass or catheterization of the aneurysm.
Second, simultaneously navigating two balloon catheters in the distal circulation may be difficult. We found it useful to navigate the balloons over a 0.012-in. guidewire (Radiofocus GT, Terumo, Tokyo, Japan) to overcome this difficulty. Besides these drawbacks, the presence of multiple catheters in small arteries compromised perfusion of the distal arteries, and we decided to administer intra-arterial nimodipine to prevent catheter-induced vasospasm.
The third issue is the potential risk of repeated balloon inflation in the distal vessels. Although the use of compliant balloon catheters was reported to be safe, even in the treatment of distal vasospasm (11), rupture of parent artery during balloon-assisted coiling has been documented with other balloon catheters during remodeling (6, 12).
Our final concern was that a bifurcation aneurysm with a neck wide enough to warrant a nonstandard technique might have been hard to visualize angiographically. Consequently, slight encroachment of coils or excessive protrusion of the balloon into the neck of the aneurysm could be missed. In our second patient, one of these two mechanisms might have played a role, resulting in the rare phenomenon (13, 14) of delayed thromboembolism. Increased surface area of exposed coils at the aneurysm–parent artery interface in wide-necked aneurysms is postulated to increase the risk of thromboembolic events or occlusion of the parent artery (14–19), and neck size may be an independent factor for such events regardless of the coiling method used for treatment (15).
The increasing placement of intracranial stents to treat aneurysms and the favorable results obtained with their use (9) suggest that stents are likely to dominate the endovascular treatment of aneurysms. At this time, stent placement is associated with problems such as thromboembolic events and stent migration (2, 8, 9) and mismatch between the smallest available stents and the size of the small parent arteries (1). Therefore, current methods of stent placement may not be best suited for the treatment of bifurcation aneurysms with a wide neck (2). Pending the refinement of stent technology, treating wide-necked aneurysms with a double-balloon remodeling technique might be possible when proper indications for such a treatment exist. We expect that low-profile, compliant balloon catheters and knowledge of potential pitfalls of the technique will decrease the complication rates of techniques involving multiple balloon catheters.
References
- Received December 29, 2004.
- Accepted after revision March 1, 2005.
- Copyright © American Society of Neuroradiology