Abstract
Summary: We present the case of a scuba diver who experienced acute ear pain during ascent from a dive. CT imaging was performed because of severe unrelenting headache. Blood and gas was identified within the epidural space of the middle fossa and over the petrous bone, as well as hemorrhage within the adjacent temporal lobe. To the best of our knowledge, this is the first case of CT-documented barotrauma affecting the brain as a result of middle-ear gas rupturing through the tegmen tympani.
Middle-ear barotrauma may occur with a rapid change of ambient pressure. A pressure gradient can develop when there is compromise of airflow through the Eustachian tube. This is most likely to affect divers or airplane passengers. There is a potential risk of intracranial injury in those with a developmental deficiency in the tegmen tympani.
Case Report
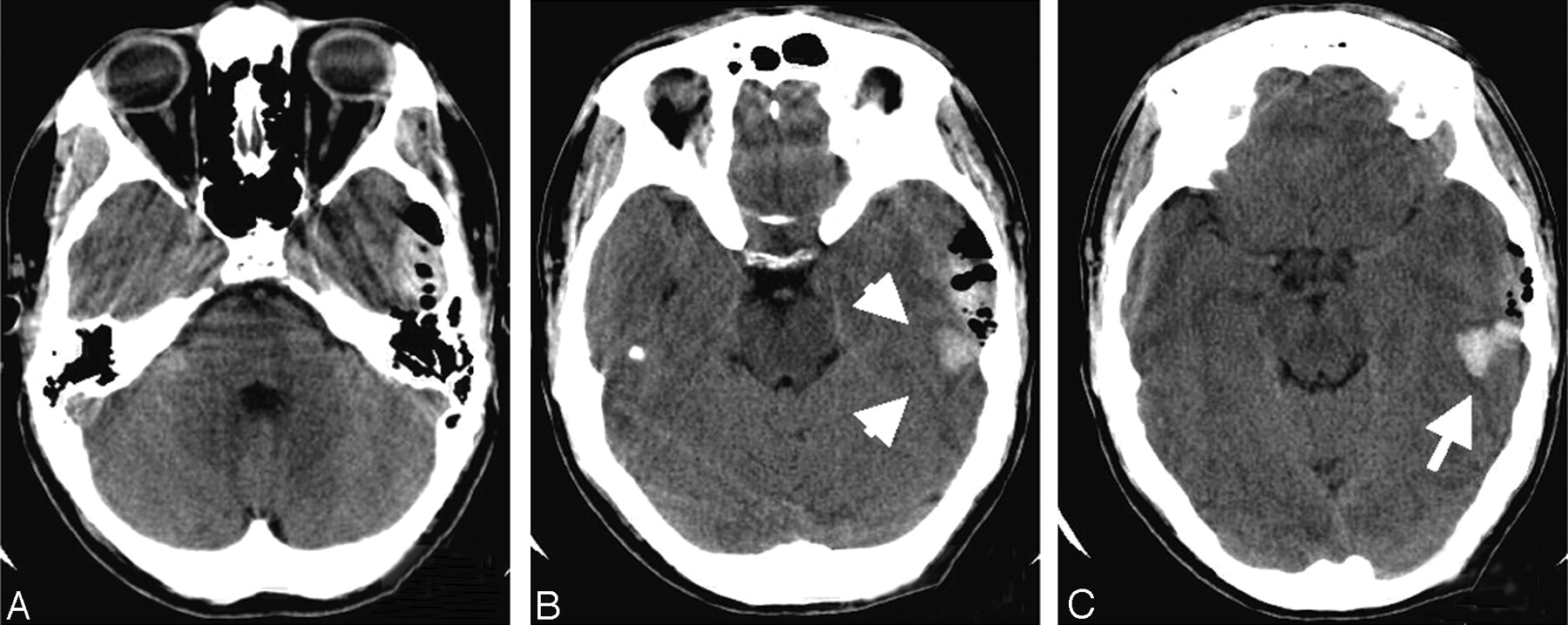
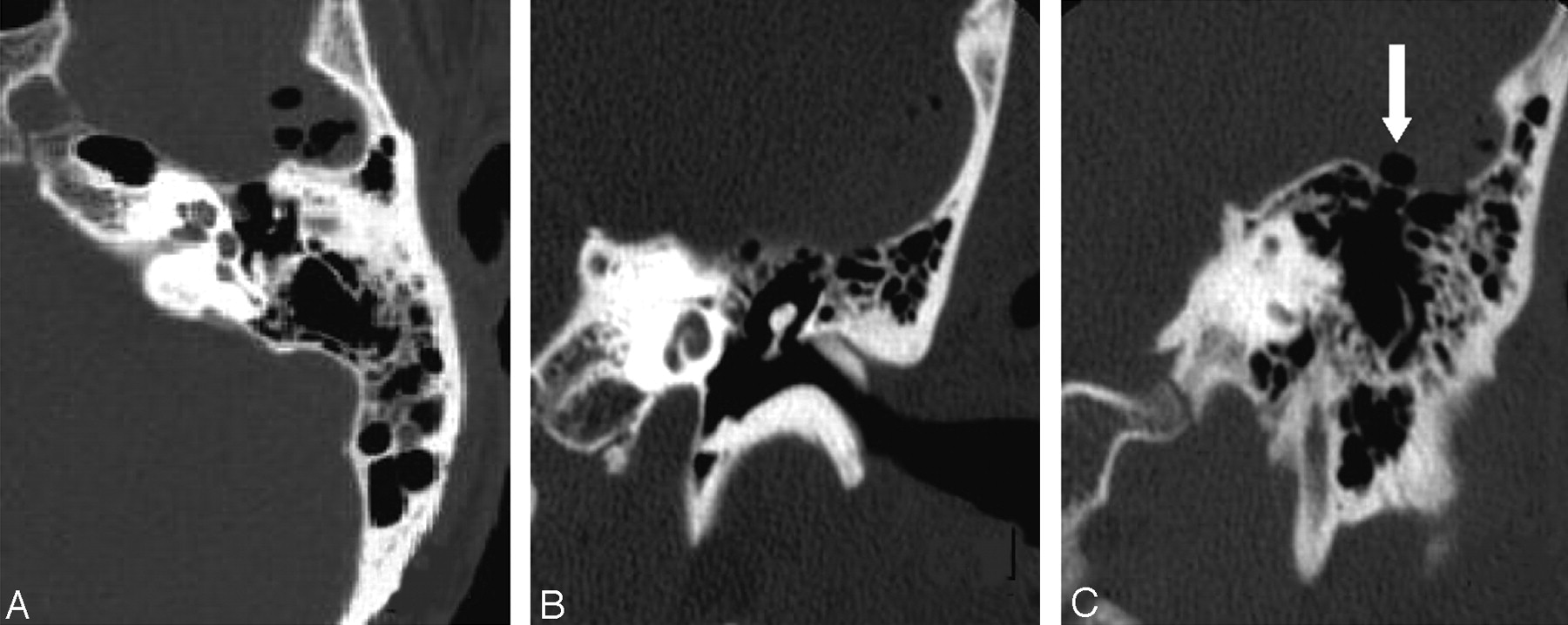
A 31-year-old man experienced severe left ear pain while ascending from a 30-foot scuba dive. At the surface, his “left ear exploded.” His instructor told him to redescend to 30 feet to “recompress,” but this did not produce improvement. He was subsequently seen at the emergency room with persistence of otalgia, decreased hearing on the left, and vertigo. His Glasgow coma scale was 15. Otologic and neurologic examinations did not reveal deficits. Continuing headache despite treatment with analgesics prompted a CT scan (Fig 1), which showed parenchymal hemorrhage within the left temporal lobe overlying the petrous bone, as well as epidural blood and gas in the middle fossa. No abnormality was seen within the temporal bone, but a high-resolution temporal bone CT scan (Fig. 2) done 24 hours after the event showed minimal opacification of left mastoid air cells without air fluid levels. No bone disruption could be identified, but bone could not be clearly identified along the entire tegmen tympani of either temporal bone. Both mastoids were extensively pneumatized.
The management of the intracranial findings was conservative. Three weeks later, after skydiving, headache reappeared, accompanied by nausea and left facial numbness. A new CT showed resolving left epidural hematoma, and investigation for meningitis was negative.
Four months after the scuba-diving accident, imbalance and subtle left tympanic membrane erythema raised the question of perilymph fistulization. An exploratory tympanotomy ruled out this possibility, and packing of the round window niche with fat was performed. A follow-up CT scan showed complete normalization 9 months after the initial event.
Discussion
Barotrauma to the middle or inner ear can occur during descent or ascent in scuba diving and reflects failure to equalize the pressure between the middle ear and the ambient pressure. Following Boyle’s law, air within the middle ear will be compressed to a volume inversely proportional to the pressure exerted by the overlying water. A 33-foot dive will double the ambient pressure from 1 to 2 atmospheres absolute. As the diver ascends, the same water pressure column decreases and release of gas from the middle ear through equalization of pressures is necessary, to compensate for the expanding volume of air (1).
If the Eustachian tube is not patent, there can be a “reverse squeeze” during ascent as pressure in the middle ear exceeds the ambient pressure. Rupture through the tegmen tympani may potentially occur, especially if the bone is thin or deficient.
Malby and Stewart (2) found tegmen tympani defects in 52% of 50 routine autopsy cases and showed that extension of air into the epidural space could occur with routine otolaryngology procedures by using a Siegles bulb or Politzer bag. Indeed, their study was prompted by the death of a 40-year-old patient within 2 hours after air insufflation via a Siegler speculum. Autopsy showed an acute epidural hematoma overlaying the tegmen. Because of rare but catastrophic cases like this, reverse valsalva and Eustachian tube catheterization are no longer in use.
Intracranial complications of middle-ear barotrauma are rare. Middle-ear barotrauma in our patient caused pneumocephalus, as well as parenchymal and extra-axial hemorrhage.
CT scanning was carried out because of severe, unrelenting headache in our patient, who had no neurologic abnormality. The presence of hemorrhage within the temporal lobe occurred secondary to significant increased pressure within the middle ear with resulting rupture of the roof of the petrous bone (2). We believe that, in our patient, the rupture may have occurred secondary to an unrecognized developmental bony abnormality or through an area of very thin tegmen tympani. Reports of spontaneous CSF leaks associated with one or more dehiscences of the tegmen tympani support this route as the potential source of communication with the intracranial cavity (3, 4).
A similar case of pneumocephalus after scuba diving has been reported by Goldman (5). He also described an epidural hematoma found on MR imaging 16 days after the injury, but no intraparenchymal hemorrhage was described in that case. He did not identify an osseous defect either.
Conclusion
Our case illustrates the relevance of neuroimaging in the detection of potentially lethal intracranial complications associated with middle-ear barotrauma, even in the absence of focal neurologic deficits.

Noncontrast axial CT obtained at time of initial presentation in emergency. Sections obtained at the level of the petrous bone (A), immediately above the petrous bone (B), and more superiorly through the temporal lobe (C) demonstrate epidural blood and gas in the left middle fossa as well as parenchymal blood (B and C, arrows) in the temporal lobe immediately above the petrous bone.
{/GRAPH;zj40050506070002;comptd;;center;stack}

{kind=link}
{kind=link}
A, High-resolution CT of the left temporal bone obtained 15 hours after the initial CT. Axial (A) and coronal (B and C) views show subtle opacification of mastoid cells and intracranial air within the middle fossa. Middle-ear cavity is normal, but gas is present immediately above the tegmen tympani (C, arrow). No disruption can be identified but bone could not be clearly identified along the entire tegmen tympani (other images not included).
Footnotes
Presented as Excerpta Extraordinaire, at the 42nd annual meeting of the American Society of Neuroradiology, Seattle, WA, June 8, 2004.
References
- Received July 16, 2004.
- Accepted after revision July 30, 2004.
- Copyright © American Society of Neuroradiology