We read with interest the recent case report by Michael Chow and the Cleveland Clinic group regarding treatment of a wide-necked basilar bifurcation aneurysm by using the Y-configuration double-stent technique (1). This report and others (2) show the enormous potential of flexible intracranial stents for therapy of complex cerebral aneurysms. As stated by the authors, however, limitations of the technique exist (3), and more will be discovered. We relate one such cautionary tale.
A 62-year-old woman was referred to our institution for treatment of a large, wide-necked basilar bifurcation aneurysm (Fig 1). Both P1 segments of the posterior cerebral arteries were incorporated in the neck. Our knowledge of the Cleveland experience and the anticipated difficulties with conventional endovascular therapies for aneurysms in this location led us to proceed with the double-stent assisted coiling approach.
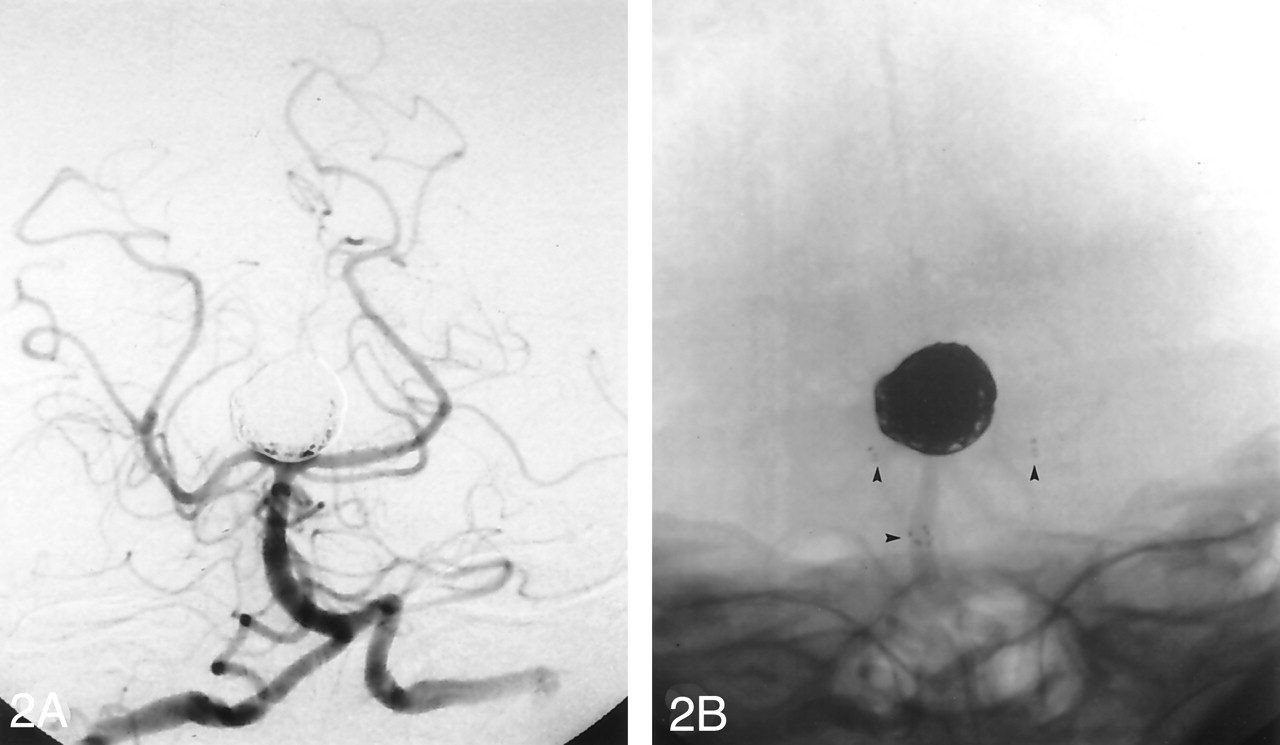
This was achieved by using two 3.5 × 20 mm Neuroform (Boston Scientific, Natick, MA) stents and 386 cm of GDC (Boston Scientific) coils in a fashion similar to the method described by Chow et al (Figs 2). The procedure was performed under general anesthesia and full heparinization, with the standard pretreatment for Neuroform cases including aspirin and clopidigrel. There was near-complete obliteration of the aneurysm with preservation of both posterior cerebral arteries and no evidence of perforation, vessel dissection, or flow-limiting stenosis. The patient awoke from anesthesia with no focal neurologic deficit; however, approximately 6 hours later, she became progressively obtunded with left-sided weakness. A CT head scan showed a midbrain and upper pontine parenchymal hemorrhage (Fig 3), and cerebral angiography showed no change from the postprocedural study. The patient had a limited neurologic recovery but eventually succumbed to chronic hydrocephalus and pneumonia.
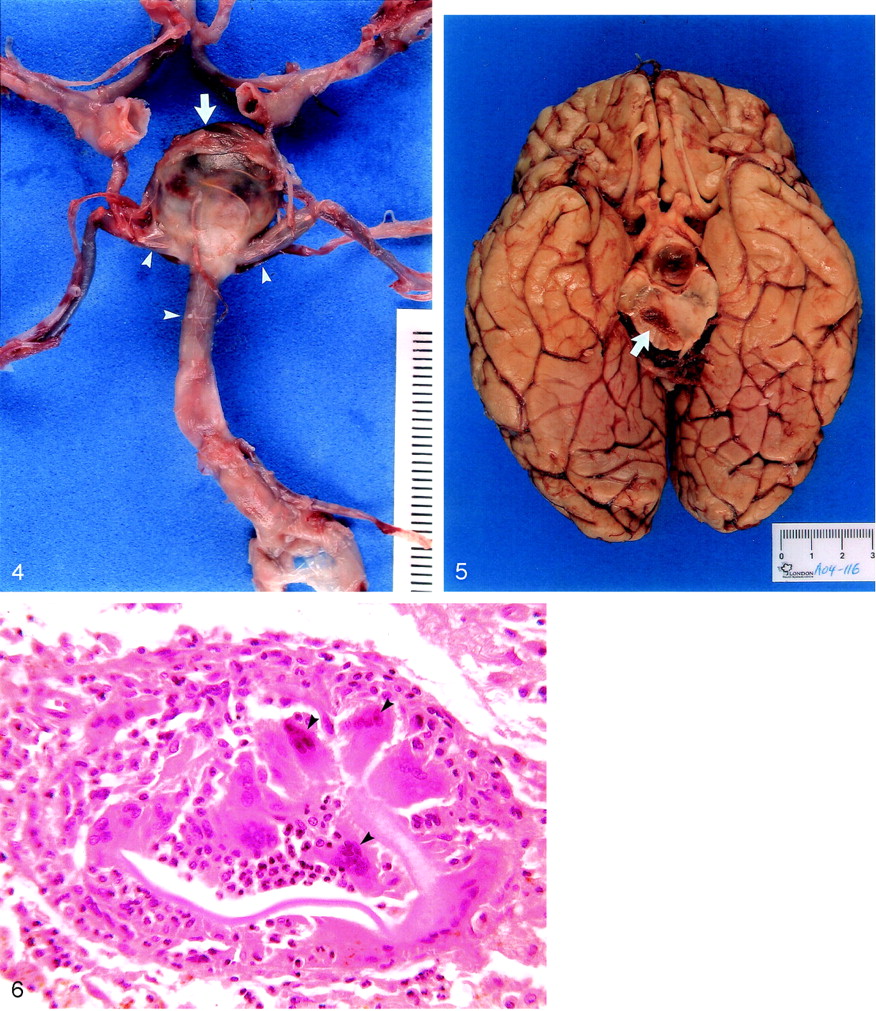
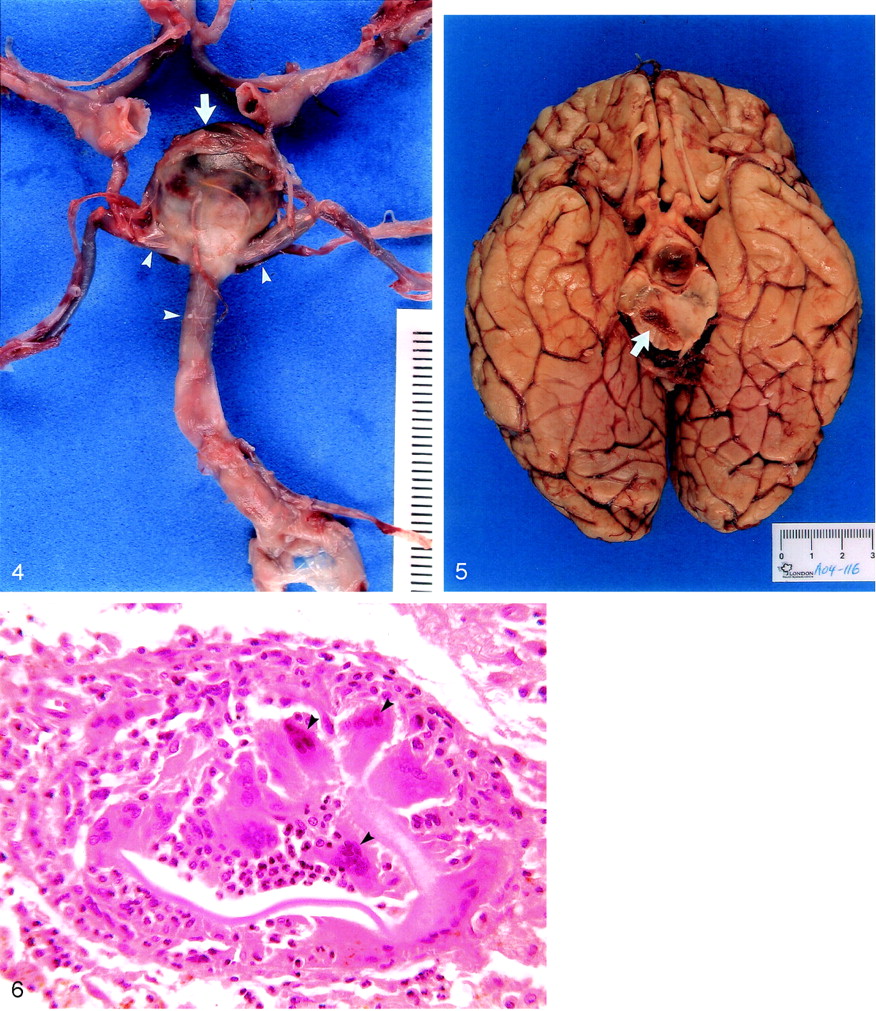
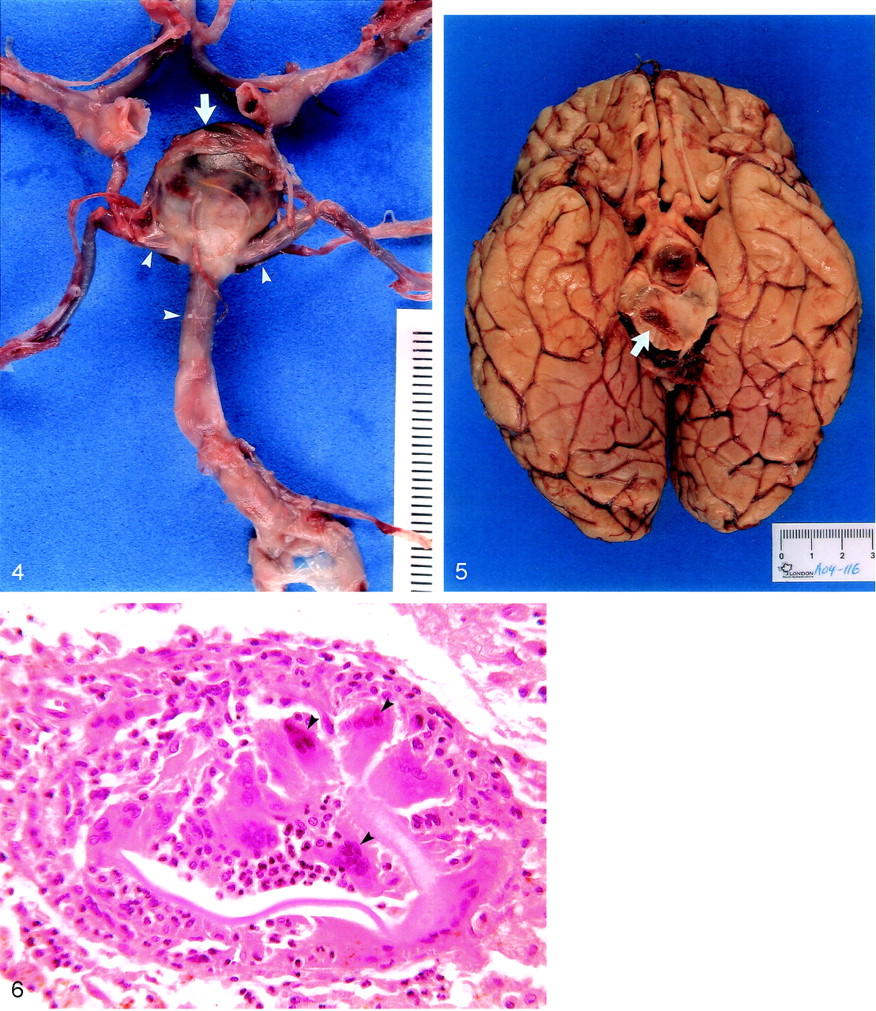
A subsequent review of the procedure showed considerable stretching of the right posterior cerebral artery during guidewire placement and positioning of the first Neuroform stent. There were no other technical problems encountered during the procedure. The postmortem neuropathologic examination showed no bleeding from the aneurysm (Fig 4) and no gross obstruction of pontine perforating vessels by the stents. There was a large right midbrain hemorrhage (Fig 5), with smaller hemorrhages in the right thalamus and right cerebellar hemisphere.
Unusual foreign body granulomas were also seen microscopically (Fig 6) associated with the hemorrhages, possibly due to microembolism from the hardware. Although the cause of the midbrain hemorrhage is unknown, it may be due to stretching of perforating vessels, infarction, and bleeding related to anticoagulation.
Despite an excellent angiographic result, this tragic clinicaloutcome demonstrates the risks inherent in novel, aggressive interventional strategies. This, however, should come as no surprise. As William Shakespeare noted long ago, Diseases desperate grown
By desperate appliance are reliev’d
Or not at all (4)

Right vertebral arteriogram (anteroposterior [AP]), shows a wide-necked basilar bifurcation aneurysm.

Postoperative arteriograms.
A, Right vertebral arteriogram (AP), obtained after treatment with stents and coils, shows near complete obliteration of the aneurysm.
B, Unsubtracted image obtained from the postoperative arteriogram shows the radiopaque markers at the ends of the stents (arrowheads).

CT head scan obtained 6 hours after treatment shows the pontine component of the acute brain stem hemorrhage (arrow).

Postmortem dissection of the circle of Willis, showing the coils inside an intact basilar bifurcation aneurysm (arrow). The stents are visible through the basilar and posterior cerebral arteries (arrowheads).

Gross specimen. Section through the midbrain shows the hematoma (arrow)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Microscopic section through the midbrain hemorrhage shows unusual intravascular foreign body granulomas (arrowheads) (H&E, ×8).
References
- Copyright © American Society of Neuroradiology