
Abstract
Summary: A 38-year-old man with Marfan syndrome presented with headache and neck pain. MR imaging revealed a large enhancing mass in the cervical anterior epidural space. Cervical laminectomy with biopsy of the lesion revealed a large engorged anterior epidural venous plexus (AEVP). Marfan syndrome may predispose the patient to enlargement of AEVP secondary to a vessel wall abnormality.
Marfan syndrome, an inheritable connective tissue disorder first described 100 years ago, has been associated with multiple abnormalities of the ocular, cardiac, and skeletal systems. The diagnosis is based on the clinical presentation and linkage to the dominantly inherited gene MFS-1 on 15q21 or the discovery of the family mutation (1). Although cases of an enlarged cervical anterior epidural venous plexus (AEVP) causing neurologic symptoms have been reported (2–4), to our knowledge, no report of its association with Marfan syndrome exists.
Case Report
A 38-year-old man with a family history of Marfan syndrome presented with an acute onset of headache and neck pain for 4 days prior to admission. The pain started from his left occiput and radiated down to his neck. This symptom was refractory to medical treatment, and the patient had no prior history of headache or head or neck injury. He did not have any signs of meningitis. He denied bowel or bladder symptoms.
Physical examination findings were notable for the classic Marfan presentation; the patient had a long, thin face; arachnodactyly (ie, long fingers); and dolichostenomelia (ie, long extremities). Neurologically, findings from the strength and sensory examination were normal in the upper and lower extremities. Reflexes were normal and symmetric, without evidence of clonus or the Babinski sign. Results of the cranial nerve examination were normal. No cutaneous lesions were observed.
MR imaging revealed a ventral epidural mass extending from C1 to C6 (Fig 1A). This mass appeared to be bilobed and was along the posterior longitudinal ligament (PLL). The mass showed relative homogeneous enhancement, with several small nonenhancing areas (Fig 1B). Slight, bilateral narrowing of the neural foramina was present through the upper and middle parts of the cervical spine near the mass; however, no sign of cord compression and no evidence of abnormal signal intensity or enhancement within the cord were observed. Dural ectasia with posterior vertebral body scalloping was noted in the lumbar spine. The differential diagnosis included an epidural abscess, hematoma, enlarged epidural venous plexus, and neoplastic process. Results of subsequent diagnostic evaluation for malignancy, infection, and inflammatory processes were all negative. MR imaging findings in the head were unremarkable.

MR images show an anterior epidural mass.
A, Sagittal T1-weighted image show a relatively homogeneous, isointense ventral mass that extends from C1 to C5.
B, Sagittal T1-weighted image obtained after the administration of gadopentetate dimeglumine (Gd-DTPA) shows a ventral epidural mass that extends from C1 to C7. Small nonenhancing areas may represent thrombosed veins.
C, Sagittal T2-weighted image shows a large hyperintense mass with punctate areas of isointensity.
D, Axial T1-weighted image obtained after the administration of Gd-DTPA shows the enhancing bilobular anterior epidural mass.
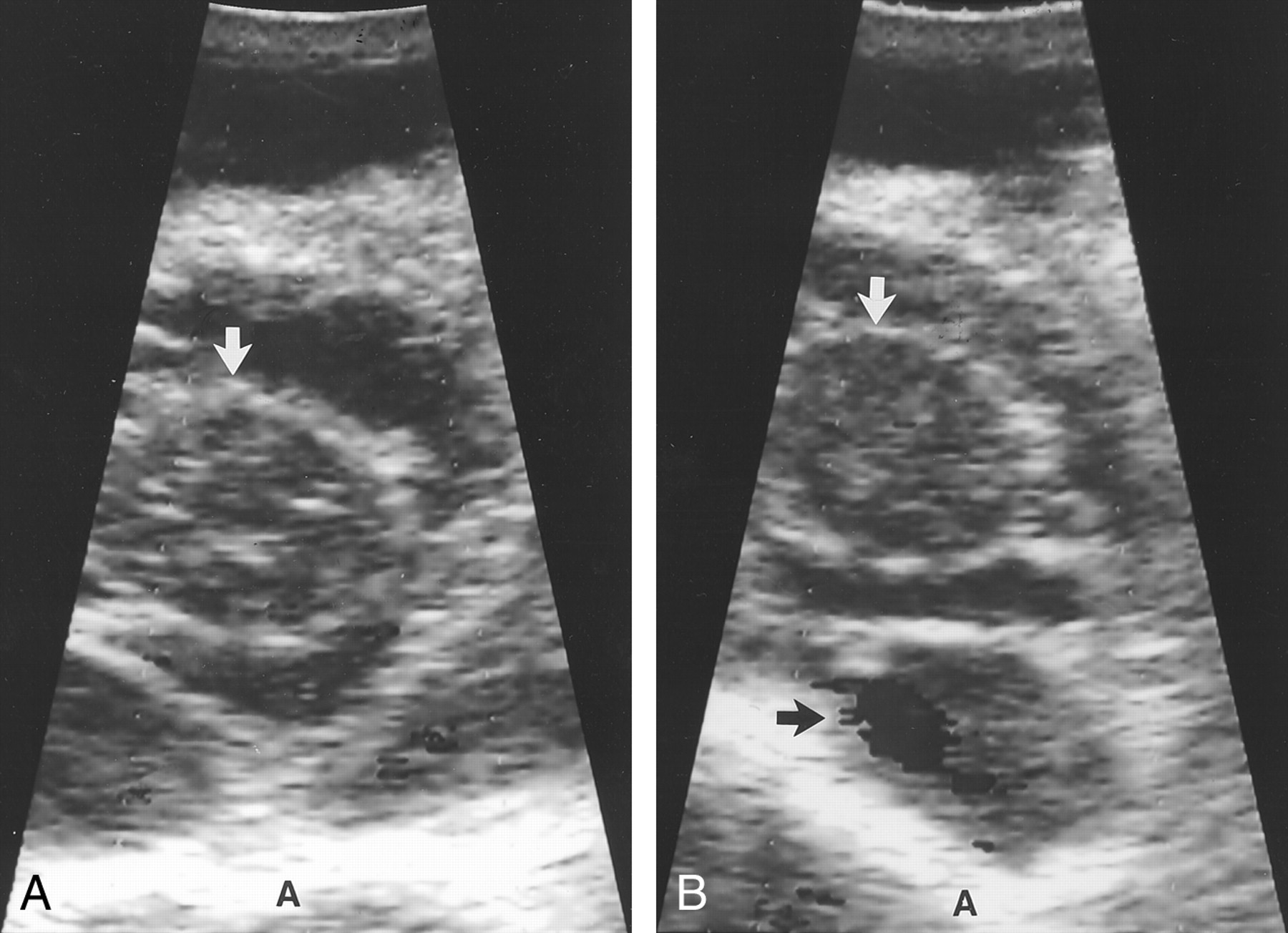
Cervical hemilaminectomy was performed at the level of C2 to obtain a definitive diagnosis. The C2 level was chosen because the mass was largest at this level. This exposure revealed abnormal tissue, which was found on the left side of the cervical canal at the anterior aspect of the dural sac. Initially, this tissue was entered, and a biopsy sample was obtained. On visual examination, this tissue appeared to be an engorged venous plexus that was partially thrombosed. Therefore, color Doppler sonography was performed in this field. Doppler sonography revealed sluggish but definite blood flow in both sides of the mass (Fig 2A). The Doppler signal was markedly enhanced, with increased venous return on the right side when the Valsalva maneuver was performed (Fig 2B). However, on the left side, a filling defect was present; this confirmed the presence of a thrombus. The left side of the dural sac was slightly compressed because of this thrombosed vein. Sonograms clearly demonstrated the absence of a mass effect on the spinal cord. Because of the complex vascular nature of the mass, no resection was performed. Analysis of the biopsy specimen revealed connective fibrous tissue with thrombus. The patient’s headaches and neck pain resolved postoperatively, and remained so at 12-month follow-up.

Intraoperative Doppler sonograms of the cervical spine. White arrow indicates the spinal cord; A, anterior.
A, Sonogram of the cervical AEVP shows slow flow in the venous plexus.
B, The initiation of a Valsalva maneuver enhances the Doppler signal within the cervical AEVP (black arrow).
Discussion
An enlarged symptomatic anterior epidural plexus is a rare finding, and only a few reports of these exist (2–4). To our knowledge, an enlarged symptomatic anterior AEVP in association with Marfan syndrome has not been reported in the literature. When an AEVP is present in the lumbosacral spine, associated symptoms include sciatica and urinary retention. Only two reports have documented symptoms of myelopathy secondary to spinal cord compression when present in the cervicothoracic region (3, 11).
Marfan syndrome has long been associated with connective tissue disorders, such as cervical bony and ligamentous abnormalities and dural ectasia (5, 6). An association between Marfan syndrome and intracranial aneurysm has also been suggested because patients with these conditions have abnormalities of the arterial wall that consist of widespread changes with intimal proliferation, medial degeneration, and fragmentation of the internal elastic lamina (7). This association raises the possibility that such changes may also involve the venous architecture, resulting in an enlargement of the AEVP that is sufficient to cause neurologic symptoms.
To date, the cause of enlarged cervical AEVP has been poorly understood, and both congenital and acquired causes have been proposed (8, 9). Enlargement may occur secondary to a herniated disc or compressive lesions in the spinal cord (2, 10). Trauma has also been implicated (2). Vascular malformations (ie, arteriovenous fistulas) are also commonly associated with enlarged epidural or intradural veins. Cases of internal jugular vein thrombosis or stenosis and superior vena cava obstructions have been documented; these conditions have resulted in dilation of the AEVP secondary to collateral venous flow from the brain via the basilar venous plexus (11).
In our case, Marfan syndrome may have predisposed the patient to an enlargement of AEVP due to a disorder of the venous connective tissue. The elastic tissue within the walls of the veins may be abnormal in Marfan syndrome; this abnormality may result in the dilation of the anterior epidural plexus, even with normal venous pressures (12). This association may contribute to the plexal enlargement, as described previously. Alternatively, Fishman and Dillon (13) noted venous engorgement in the setting of a spontaneous CSF leak that was attributed to a reduced CSF volume. Similarly, lumbar ectasia, which is commonly noted in Marfan syndrome, may result in an enlarged subarachnoid space. This effect may be worse in the standing position, which causes the CSF to pool in the lumbar region. This pooling results in a relatively negative CSF pressure in the cervical region, which leads to the progressive dilation of the venous plexus as a compensatory phenomenon.
Radiographically, about 25% of cervical AEVPs can be visualized on nonenhanced MR images, and 89% are depicted on contrast material–enhanced images. Gelber et al (14) noted that, when visualized, the plexus measured 1–3 mm; in their series of 70 cases no plexus had a diameter of greater than 4 mm. The plexus is usually not visualized in the midline because the posterior longitudinal ligament is well opposed to the vertebral body, (15) and it usually becomes progressively attenuating below C2-C3. In our case, the cervical AEVP appeared enlarged (measuring 6 mm maximally), and it had inhomogeneous contrast enhancement, which was probably related to the partial thrombosis found during surgery.
Management of these rare lesions includes simple decompressive laminectomy; laminectomy with resection of the enlarged cervical AEVP (10); and, in one case (11), a sigmoid sinus–to–internal jugular vein bypass to decompress a dilated epidural venous plexus. Symptoms of radiculopathy and myelopathy generally improve in these cases. We elected to perform simple decompressive hemilaminectomy with intraoperative sonography. The presence of flow and marked enhancement of the Doppler signal with a Valsalva maneuver confirmed the venous nature of the lesion. Decompressive hemilaminectomy prevented the profuse bleeding associated with resection of the venous plexus. Additionally, a possible risk of venous congestion was avoided, secondary to the loss of venous drainage via medullary veins in the spinal cord and basilar venous plexus. Whether surgical decompression was sufficient to resolve the symptoms is unclear. Alternatively, the cause of the acute pain may have been the venous thrombosis that resolved over time, regardless of surgery.
Conclusion
In summary, our report describes symptomatic AEVP in a patient with Marfan syndrome. This case raises questions about whether Marfan syndrome predisposes the patient to the formation of an enlarged AEVP. It also illustrates the importance of including a dilated AEVP in the differential diagnosis of a ventral epidural mass in the cervical spine. Awareness of this possibility may prevent inadvertent percutaneous or surgical biopsy. Intraoperative Doppler sonography also has an important role in this regard because it demonstrated the vascular nature of the lesion. On imaging, these structures can have nonhomogeneous contrast enhancement, even in the absence of thrombosis, due to the slow flow.
References
- Received June 15, 2001.
- Accepted after revision October 23, 2001.
- Copyright © American Society of Neuroradiology
In this issue





{kind=link}
{kind=link}
Jump to section
Related Articles
Cited By...
- No citing articles found.