July 2016
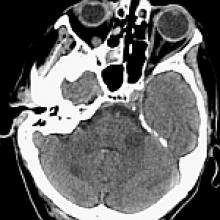
A 72-year-old woman with 3-month history of daily headaches presents to the ER with subacute onset of nausea, vomiting, speech difficulties, and impaired gait.
AJNR Awards, New Junior Editors, and more. Read the latest AJNR updates
A 72-year-old woman with 3-month history of daily headaches presents to the ER with subacute onset of nausea, vomiting, speech difficulties, and impaired gait.