June 30, 2022
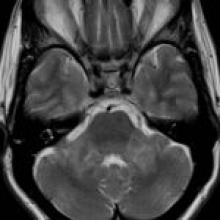
A 56-year-old woman with a several-year history of progressive dizziness, hearing loss, diplopia, gait instability, emotional lability, and fatigue
AJNR Awards, New Junior Editors, and more. Read the latest AJNR updates
A 56-year-old woman with a several-year history of progressive dizziness, hearing loss, diplopia, gait instability, emotional lability, and fatigue