November 2022
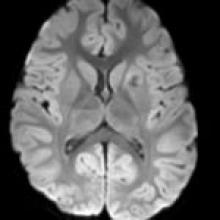
A 3-year-old girl with developmental delay presents with seizures refractory to multiple antiepileptics.
AJNR Awards, New Junior Editors, and more. Read the latest AJNR updates
A 3-year-old girl with developmental delay presents with seizures refractory to multiple antiepileptics.